4 May 2021, by Jolijn Santegoeds, www.mindrights.nl
The history of European mental health care calls for a reflection on the doctrine of ‘normalcy’.
This article provides many reasons to campaign against the Council of Europe’s Draft Additional Protocol to the Oviedo Convention. #WithdrawOviedo #StopForcedTreatment https://www.withdrawoviedo.info/join
Various events throughout European history have impacted on the mental health care sector, and this history has contributed to the development of practices in European mental health care up to today.
This is a long and detailed article about shocking practices and events which impacted European mental health care directly or indirectly, such as MK Ultra, Operation Paperclip, World War 2 and torture in mental health care. This article presents an outline of the need for change in European mental health care to meet human rights standards.
Initially, my interest was caught by the historical, unethical project called “MK Ultra”, which took place in the aftermath of World War 2, in the context of the Cold War. The secrecy of the MK Ultra project has often given rise to unclarity and speculations, and even sparked conspiracy theories. It’s a complicated and delicate matter, and it’s a painful part of the history of the world. During my exploration of the impact of MK Ultra, I came to the conclusion that the professional development of European mental health care in fact has gone fundamentally wrong at various points in history.
At present, Europe has a chance to break away from its dark past, by making sure that the Council of Europe’s Draft Additional Protocol to the Oviedo Convention will not be adopted. This article will motivate why Europe must ban institutionalization and coercion from mental health care.
MK Ultra
MK Ultra stands for a highly controversial research project on “mind control” by the US, in which it used knowledge obtained by World War 2. The infamous MK Ultra project with 149 subprojects was carried out in the period of the Cold War between 1950 and 1973, with some projects overlapping and continuing under other code names, such as MKSEARCH, MKNAOMI, MKDELTA, MKOFTEN, Bluebird, Artichoke, Stargate, QKHILLTOP and other names. It is unclear if it has fully ended, or possibly has been taken on in other projects into later decades.
The most known experiments are those in the USA where the drug LSD was distributed to test persons without their consent. Yet the MK Ultra project carried a much larger scope. MK Ultra used a spectrum of techniques to manipulate mental states and brain functions, including by psychoactive drugs (especially LSD), paralyzing drugs and other chemicals, electroshocks, hypnosis, sensory deprivation, isolation, high temperatures, brain damages, and verbal and sexual abuse, and other forms of torture, in order to develop a better understanding of how to destroy and to control human minds. Abusive studies under mental health care to assert control over the mind and behavior of people were a substantial part of the decades-long study to control the human mind.
The scope of Project MK Ultra and related projects was broad and outright horrifying. MK Ultra was simultaneously performed with many other operations and warfare experiments, such as for example experimentation with biological warfare (bacteria, viruses, cancer, fleas), chemical warfare (VX and Sarin, Operation Tophat). From 1951 to 1974 the Holmesburg prison program studied the dermatology and health effects of dioxin and other herbicides, and from 1962 to 1971 under Operation Ranch Hand, the Rainbow Herbicides were used on Vietnam. Also there were nuclear tests under Operation Gabriel, Sunshine, Plumbbob (radioactive radiation exposure tests, and e.g. giving radioactive food to children with mental disabilities), and experimentation on animals. MK Ultra activities were carried out under the guise of research in institutions, hospitals, prisons, and other places such as secret detention centers in Europe and East Asia, and CIAs involvement was often not known. MK Ultra experiments were often performed without consent of the persons subjected, and were in blunt violation of the 1925 Geneva Protocol which prohibits the use of chemical and biological weapons in war. The head of the CIA ordered to burn the reports of MK Ultra in 1973.
Many of the torture techniques developed in the MK Ultra studies and other programs were later used in prisons such as Guantanamo Bay and Abu Ghraib.
Use of ‘war intelligence’
Another highly disputed part of MK Ultra was the use of so-called ‘war intelligence’ obtained through projects such as “Operation Paperclip” after World War 2. After the liberation of Europe from the Nazi regime, the US, Russia and other countries collected thousands of scientists and leaders (including from the Nazi Party), who were given high level positions abroad. “Brain drain” it was called, and it supposedly served to prevent the oppressive regime from repeating itself. Yet, the fact that these ‘inventors of the Holocaust’ got high ranking positions with fame and fortune abroad remains utterly painful, and calls for reflection.
Holocaust
The Nazi regime of Germany executed a terrifying range of cruelties on its population, by systematic mass murder on Jewish people and other minority groups, who were deported to concentration camps where they were subjected to torture, slavery, starvation and death. Millions of people were killed. The Nazi regime used propaganda as a means to ‘normalize’ the organized abuse and violence against Jews and other groups in the community, which were accused as ‘unworthy of living’. Under the doctrine of eugenics, many residential institutions were forced to become sites of forced sterilization, experimentation and starvation, since the Nazi regime also did not recognize the person with disabilities’ equal right to life or reproduction.
Obviously, the leaders and enablers of the Nazi regime were war criminals, and should have been treated as such. Operation Paperclip feels unfair. After the capitulation of Nazi Germany there were 3,4 million prisoners of war who were held at 19 locations of secured meadows with barbed wire near the river Rhein under appalling conditions (“Rheinwiesenlagern”). They all suffered and thousands of people died. The contrast is huge with the leaders who escaped their responsibilities and got a new career.
It is hard to understand why MK Ultra and Operation Paperclip could go with impunity up to today.
A thorough reflection on the context of MK Ultra and the global situation of past century may shed a light on why projects such as Operation Paperclip and MK Ultra could take off and go with silence.
World War 2: Axis, Allied and United Nations
During World War 2, the Axis (Nazi Germany, Italy and Japan) were expanding their territory over nearly all of Europe, a part of Northern Africa and a part of East Asia near Japan. In response, several other countries, such as the UK, China, US, Soviet Union and Canada formed a counter force: the Allied. Amongst the Allied there was a strong feeling that an international organization was needed to foster peace amongst all nations, and in 1941 the Declaration of St. James Palace stated: “the only true basis of enduring peace is the willing cooperation of free peoples in a world in which, relieved of the menace of aggression, all may enjoy economic and social security”, which formed the basis of the human rights principles, the Declaration of the United Nations in 1942 and the founding of the United Nations in 1945.
The European Axis (Nazi Germany and Italy) were defeated by the Allied in May 1945. Japan suffered 2 atom bombs in August 1945, leading to its capitulation which brought World War 2 to an end. The Allied had given their lives for our freedom, which is the biggest gift ever, for which we are still very grateful every day. The horrible war costed the lives of millions of people. The price for our freedom was very high. The United Nations brought hope for peace amongst the nations.
“Brain drain”
After the war, Germany was split up in “Bundeslander” and was placed under supervisory occupation by the UK, US, France, Norway Belgium, and Russia, to guide Allied-occupied Germany in the recovery from the war, generally in the form of a silent authority supervising daily life. In addition, the occupiers were free to take goods from their occupational territory as a compensation. For example a lot of German equipment was transported by train to Russia, as well as German scientists under Operation Osoaviakhim of the Soviet Union, which was comparable to Operation Paperclip by the US.
Cold War: competition East and West
After World War 2, the Cold War arose over a disagreement amongst the Allied-occupiers of Germany over the currency to be used in Germany, which eventually led to the division of Germany and the division of Europe in East and West by the “Iron Curtain”, which again caused agony to the population.
Between 1948 and 1952, the economic assistance program “the Marshall plan” was launched to support the rebuilding of Europe, which enabled Germany to use their new currency (German Mark).
During the Cold War, between 1945 and 1991, the US and the Soviet Union were antagonists, competing on nearly every domain and showing off their power, seemingly to intimidate each other, which was e.g. visible through nuclear and military arsenal development, but also through embargoes, propaganda, espionage, rivalry, psychological warfare, and technological competition such as the Space Race. Secret intelligence agencies still played a major role in this ‘proxy war’, and therefore the secret services showed an increasing interest in these sectors.
The Cold War in fact opened the door for competition between Operation Osoaviakhim of the Soviet Union and Operation Paperclip of the US, which may be a reason why scientists and leaders of the Nazi regime gained honorary positions abroad, to carry out a signal of a threat of tyrannical powers, as part of a competitive climate between East and West.
In 1986 the Soviet Union initiated political reforms (glasnost and perestroika) and revolutions arose in Eastern Europe, which led to the fall of the Berlin Wall in 1989 and the end of the Iron Curtain in 1991, by which the Cold War officially ended.
Colonialism: Western hunger for power
It is worth to note that at the end of World War 2 in 1945, colonialism was not banned and many Western countries still had occupied territories all over the world. The UK’s “Commonwealth” still occupied many countries e.g. in East Africa (Uganda, Kenya, Tanzania, Rhodesia, Northern Rhodesia, Bechuanaland), Sudan, Nigeria, Gambia, Sierra Leone, Gold Coast, parts of India, Pakistan, Sri Lanka, Burma, Palestine and British Malaya amongst others. The Netherlands still occupied e.g. Indonesia, a part of India, Surinam and the Antilles. France still occupied many countries in North Africa, West Africa, Equatorial Africa, Madagascar and Indochina (Laos, Cambodia and Vietnam). Portugal still occupied Angola, Mozambique, a part of India, East Timor and Macau. And the list goes on, showing that before World War 2, many countries had in fact shown a mindset of imperialism and rivalry, and pursued a hunger for power and world domination, subjecting other regions to their control.
Slavery and mass exploitation
Populations in colonized territories have also been subjected to horrific atrocities and tyrannies committed by the colonizers, which were mostly north-western European countries as well as some Asian countries, who were invading territories to obtain its resources such as oil, textiles, gold, food and the trade routes such as harbors, tracks and passes. Slavery and deportation bear similarities to the mass exploitation of subjected minorities in the Nazi working camps, as it displays a similar fundamental inequality, discrimination and inhumane exploitation, leading to masses of people living in excruciating suffering, in fear of death, and subjected to dominating powers preventing them to speak or act for themselves. The lack of recognition of slavery and north-western imperialism is still a global human rights scandal.
Independence and Civil rights
After World War 2, the countries affected by the war restored their borders and their independence through post war resolutions in cooperation with the United Nations. This in turn empowered colonized countries to reiterate their demand for their independence in the same vein. The efforts for decolonization all over the world were supported by the United Nations, which actively contributed to changing the atmosphere between states to a more respectful and constructive cooperation.
In the 1950s and 1960s the Civil Rights Movement against racial discrimination arose in the US, which inspired people in many countries all over the world to stand up for their rights and demand an end to slavery. This gave a further push to the empowerment and liberation of oppressed groups, their struggle for independence, and to the development of human rights around the world.
The process of liberation from colonial regimes, racial discrimination and slavery was and is part of a global discourse of freeing the world from oppression, in line with the hopes of the United Nations.
Propaganda and psychological war
In Europe after 1945, the Cold War emerged as a psychological war between East and West, fueled by the hostile climate of competition with the threat of tyrannies and violence, which gave rise to increased activities of espionage, infiltration, intimidation, extortion, and torture by secret services. Over the course of history of World War 2 and the Cold War in Europe, propaganda had played a crucial role in creating a culture of mass murder and genocide. Propaganda promoted views to nullify other people, and was in violation of the basic principles of universal human rights, equality and nondiscrimination.
In response, the secret services sought to develop operations to enhance their knowledge and skills on influencing public opinion and e.g. also infiltrated in main stream media to influence public opinion (Operation Mockingbird). In addition, projects such as MK Ultra focused on mind control, on influencing behavior, including a wide range of torture, such as the search for a ‘truth serum’ for which various substances were tried on human beings under MK Ultra. Yet also intoxication, hypnosis, ‘brain washing’ and brain damaging, were part of operation MK Ultra. Children were used for experimentation. Operation Midnight Climax involved using sex workers for spying purposes. And frankly, the range of experimentation under MK Ultra and related programs was actually limitless. The army operations were classified, and the exact scope and execution of MK Ultra and related programs were never fully revealed. The reports were burnt in 1973 by order of the head of the CIA.
MK Ultra in itself was part of a much larger series of US and Soviet army operations and shockingly destructive experimentation during World War 2 and the Cold War. It had been generally agreed that a new war had to be prevented at any cost, yet the Cold War and its methods also sparked huge debates, such as over the legitimacy MK Ultra and Operation Paperclip. By 1991 this psychological war ended.
Silent suffering and impunity
There has been no recognition for the horrors committed under MK Ultra and related programs and operations which subjected defenseless people to atrocious experimentation in full secret. Yet up to today, the remnants of this horrible past still echo through mental health care around the world. The betrayal, misinformation, rigid regimes and lack of trust were once installed have never been fully dismantled, since they have not been exposed as wrongdoings, but rather could go unnoticed as if it were just another day in the mental institution. This is outrageous. The silence is deafening.
Decades of abuse of the mental health sector
Throughout the past century, the wars had impacted European mental health care in various ways. During World War 2, the Nazi regime had tyrannized the psychiatric sector in atrocious ways as sites for systematic starvation, sterilization and horrible experimentation on defenseless people. And after 1945 while the rest of community enjoyed the liberation, the sector mental health care again faced abuse and exploitation under the Cold War, to feed into the psychological warfare, by studies on mind control, to be used in intersection with espionage and torture.
Under MK Ultra, programs and experiments were designed to assert control over minds and behavior through e.g. manipulation and torture, leading to covert and illegal experiments to study and program the mind with amnesia, dissociation, schizophrenia, or test the human limits and confessions under torture etc. and by studying the effect of electroshocks, repetitive sounds, drugs, solitary confinement, coma and brain damage etc. The experiments on human beings were disguised as purely technical, medical or necessary research. The experiments in mental health care under MK Ultra without the consent of the persons concerned are severe violations of human rights.
‘Planted research’: corrupted science
The secret services have actually sabotaged the development of a meaningful evidence base in mental health care, by ‘planting research’ and paying for the researches of their interest while wrapping these up as actual scientific discourses, which deformed the curriculum of research and science. In its very essence, this means that the entire scientific basis of professional mental health knowledge has been corrupted.
Continuing rhetoric of oppression
In 1950s and 1960s, as one of the leading persons in the field of psychiatry, Donald Ewen Cameron (‘proxy Paperclip’ member), was involved in MK Ultra subproject 68, and executed experiments in Montreal with e.g. electroshocks, endless repeated messages on looped tapes, drugs like LSD, paralytic drugs, and insulin induced comas. The experiments were done in an attempt to reprogram schizophrenia. Cameron was also chairing the American Psychiatric Association (APA) in 1952-1953 and the World Psychiatric Association (WPA) from 1961 to 1966. Cameron believed mental illness was a socially contagious disease which had to be detained and hence he pleaded for psychiatry as a mechanism of social control.
Unfortunately, at present, remnants of views like Donald Ewen Cameron’s are still present in various practices throughout the world, e.g. in Article 5.1.e of the European Convention on Human Rights, dating from 1950, which adopted the alignment of mental health with contagious diseases under 5.1.e concerning “the lawful detention of persons for the prevention of the spreading of infectious diseases, of persons of unsound mind, alcoholics or drug addicts or vagrants”.
Classification of ‘mental disorders’
Also, the Diagnostic and Statistical Manual of Mental Disorders (DSM) with its first version dating from 1952 is not informed by a human rights view. The DSM takes an outdated approach to classification, which inherently assumes that persons with psychosocial problems are ‘disturbed, mentally ill and incapable’ in various gradations. The perception of psychosocial suffering as part of the human spectrum of emotions and as part of human diversity cannot be united with the DSM approach, because the DSM explicitly focusses on a supposed ‘deficit’, while the focus should be on the potential of the person.
The diagnostics listed in the DSM are adopted by voting by a group of psychiatrists, since there are no objective tests or qualifiers to measure the supposed mental illnesses. Classification under DSM is also not based on a functional assessment to identify what is needed to foster inclusion, but classification is based on clustering symptoms into a diagnosis to forecast a presumed gradation of incapacity and dependency, ignorant of the potential of the person concerned. Once diagnosed with a mental illness, the status may haunt the person for the rest of his/her life. The status can be more disabling than the mental health problem.
Up to today, the DSM is considered the major handbook for mental health professionals, and has formed the basis for the current classification of ‘mental disorders’ since 1952 up to the present DSM5 and ICD11. And despite the fact that individual mental health care workers may have good intentions and may make genuine efforts to support the person, the DSM system of classification of ‘mental disorders’ is in practice turning out as a justifier for the deprivation of rights.
‘Dangerousness to society’
The conceptualization of present mental health care has been largely based on the conceptualization of psychiatry in the past, which was oriented on exclusion in institutions “to protect society”. The semantics and rhetoric of dangerousness for society and a claimed need for exclusion have been conceptualized throughout basically all mental health laws and previous lunacy laws in the north west of the world (Europe and US). These laws were proliferated to other countries e.g. in the global south. These old notions of psychiatry actually constitute discrimination on the basis of disability.
Dangerousness is not linked to psychosocial disability, which can easily be seen from the fact that e.g. not everyone with a certain diagnosis turns violent, and similarly, not all crimes are committed by persons with a diagnosis. So dangerousness is actually not depending on mental health status, yet dangerous depends largely on the circumstances of the persons such as perceived threat or safety.
A similar rhetoric of ‘impossibilities’ due to e.g. incapacity or dangerous outcomes was actually claimed also in other human rights battles in the past, such as in regards to the abolition of slavery, and with the introduction of women rights and children rights. History has already shown that dangerousness does not depend on race, gender or health. Tying assumptions of dangerousness to certain types of disabilities is discrimination and hate speech.
‘Burden to society’
Even at present, the rhetoric of ‘burden to society’ is still promoted through wordings such as “burden of disease”, which seems to suggest a lack of willingness to invest in every life, as if it would be ‘too expensive’. It is outrageous to hear such words in Europe, after the Allied gave their lives for our freedom. In the European society, everyone should be welcome and a disability is not ‘too much of a burden’ to society.
Besides that, the social-economic priorities in Europe should be recalibrated, and the neoliberal unequal distribution of wealth and resources should be remedied, before jumping to conclusions on affordability of support throughout Europe. So many times in history, persons with disabilities faced austerity measures to save big companies from economic crises. The present humanitarian crisis in mental health care, comprising systematic discrimination, exclusion and human right violations, exacerbated by the Covid-19 pandemic, necessitates making economic investments in the rights of persons with disabilities.
For ages, persons with psychosocial disabilities have been pushed to the very margins of society, and their rights have been overthrown by unfounded claims on supposed ‘safety of society’ for as long as anyone can remember. They were subjected to regimes of detention and exposed to torture by practices such as restraints, electroshocks, solitary confinement, drugging and even illegal experiments and warfare, all of which caused immense suffering to each individual subjected. In every scenario they were left neglected, and prone to bullying and violence. Such a tyrannizing regime, in such a state of powerlessness, without support, and without any recourse by the official authorities, actually meets the definition of torture. Preventing torture is in fact a core obligation under each and every human rights treaty, and a core value of the United Nations, as well as an inherent founding principle of the Council of Europe amongst others. Any unwillingness to remedy the suffering at present would actually indicate a lack of insight in mental health and human rights.
‘Need for treatment’: an excuse for institutionalization
In mental health legislation all over the world, dangerousness is being associated with on mental health problems, which portrays ‘danger to self or others’ as an intrinsic personality trait, suggesting it were ‘causally connected to mental illness’, which is actually a perception based on stigma and stereotypes. Yet, based on this prejudice, systematic preventative detention regimes have been considered legally justified under nearly all mental health laws around the world, leading to large scaled institutionalization. Yet, shockingly, inside many institutions there is no actual meaningful treatment, and in many cases, there are not even humane conditions. The Covid-19 pandemic further illustrates that institutions are not safe places.
The leading global authorities on mental health care (such as World Psychiatric Association, World Federation for Mental Health, Global Mental Health movement) have let this injustice happen, for decades in a row. The DSM classifications of “mental disorders” have been used to deprive persons of their right to be an equal member of the community. The claimed ‘need for treatment’ was in fact a covert excuse for exclusion and institutionalization.
Evidence actually shows that exclusion, institutionalization and coercion do not foster wellbeing or recovery, but rather cause suffering and an increase in psychosocial problems. There is a fundamental difference between coercion and support. Modern human rights based mental health support practices focus on wellbeing, empowerment and inclusion, and respect the will, choices and preferences of the person concerned. Psychosocial support can be provided at any location and does not have to be linked to an institution at all.
Reforms of the mental health care system in line with the UN Convention on the Rights of Persons with Disabilities (UN CRPD) are on its way, with notable developments in e.g. Peru and Ireland.
The ablist doctrine of ‘normalcy’
The European mental health sector is in fact characterized by a strong focus on ‘normal’ and ‘abnormal’ behavior, and in the past century mental health care generally aimed to ‘delete abnormal’, which is actually showing ablism. ‘Ablism’ divides the population into abled persons and disabled persons, similarly to how racism divides the population upon race and skin tone.
Systematically labelling people as ‘sick, incapable, dangerous, a burden etc’ actually has the same effect as propaganda, and is called hate speech. The media, the DSM, the globally leading professional organizations, the national laws and even the Council of Europe with their Draft Additional Protocol to the Oviedo Convention, are in fact all perpetuating ablist hate speech. There is a truly widespread doctrine which promotes ablist views on ‘normalcy’ in mental health care and in the community, which seems to aim to ‘wipe out psychosocial disability’ even against the persons will.
The intolerance towards the existence of psychosocial disability is discriminatory in itself, and clashes with the right to be free from discrimination on the basis of disability. Respect for diversity requires respecting persons with disabilities as equal members of the community, with equal rights and freedoms, regardless of disability, and entitled to an equal right to free and informed consent to any health care treatment. Forced treatment is not acceptable and constitutes a violation of human rights.
UN Convention on the Rights of persons with Disabilities
Nowadays, the word disability does not refer to supposed impairments or defects in the person, but in line with the modern notion of equality and inclusion, the term disability refers to barriers in the interaction with the community which may prevent a person from enjoying equal inclusion. Support can be needed to overcome the disabling barriers. A failure to provide reasonable accommodation is a failure of inclusion, and is therefore considered as an act of discrimination.
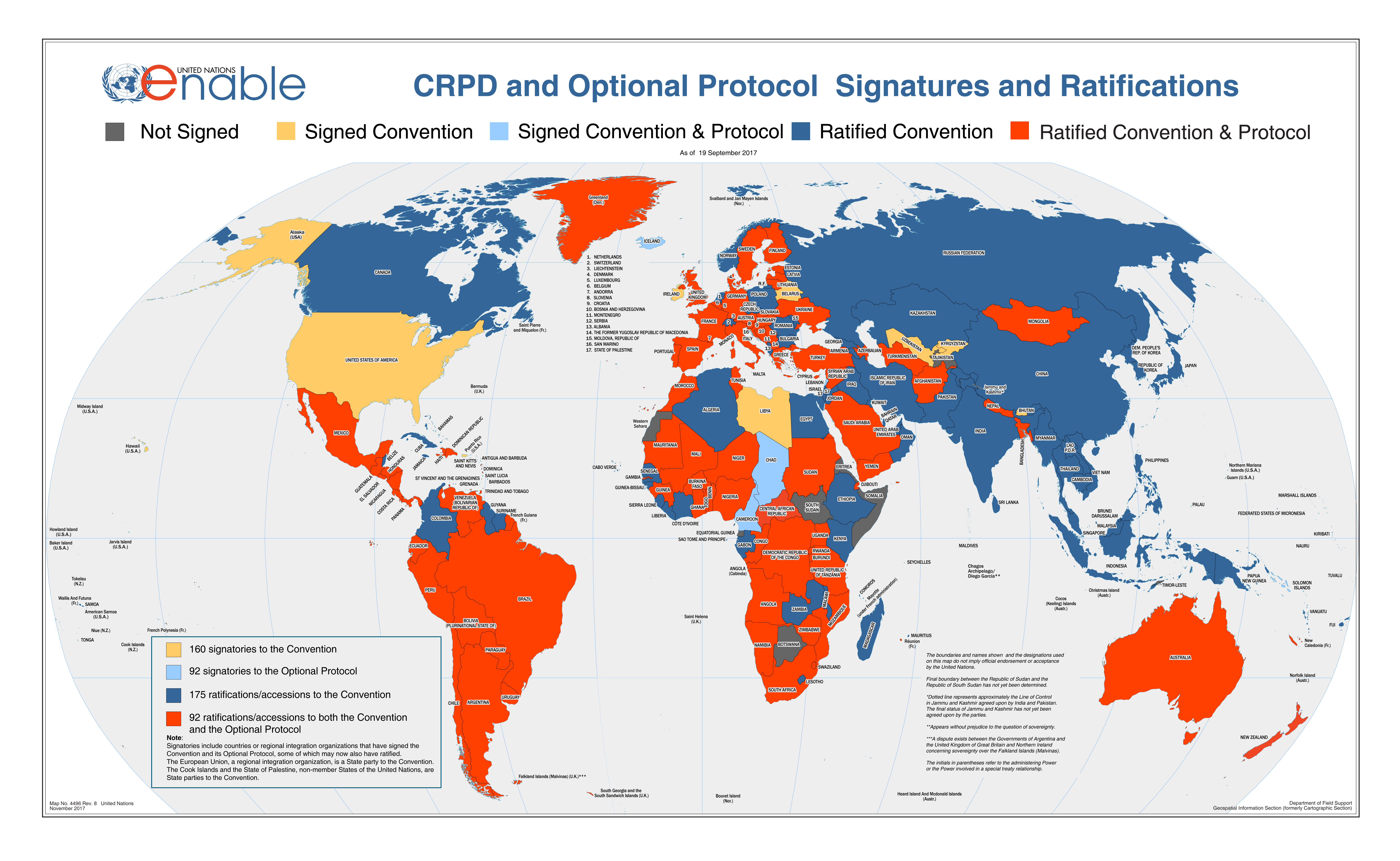
The UN Convention on the Rights of Persons with Disabilities (UN CRPD) highlights that persons with disabilities are equal members of the human family and are entitled to the enjoyment of the full spectrum of human rights on an equal basis with others. The UN CRPD provides persons with disabilities a legal tool to demand their rights to be respected on an equal basis with others, including the right to exercise their legal capacity, the right to liberty, freedom from violence exploitation and abuse, freedom from torture and ill treatment, the right to living independently and being included in the community, the right to marry and found a family, equal enjoyment of sexual and reproductive rights, free and informed consent on health care, and an adequate standard of social protection.
Ending institutionalization and repealing coercion
The UN CRPD Committee has repeatedly called for an end to institutionalization and involuntary treatments. Every person has the right to be included in the community. The UN CRPD Committee highlights the need to realize support and services in the community to foster inclusion of persons with disabilities in the community on an equal basis with others. Every person has the right to support and to the enjoyment of the highest attainable standard of physical and mental health.
Europe must act now
Europe actually still has a long way to go to before the human rights of persons with psychosocial disabilities are realized. Institutionalization must end, coercion be repealed, the doctrine of ‘normalcy’ must be banned, and arrangements of support in the community must be focused on the needs and wishes as expressed by the person concerned. A culture shift is needed in European mental health care, from exclusion to inclusion.
Despite existing norms, regulations, safeguards, guidelines, the number of persons subjected to institutionalization and forced treatments is on the rise across Europe, which shows there is an underlying problem. So far, the projects to reduce coercion generally have had a limited effect, since they could not change the entire chain of mental health care services. Real fundamental reforms are needed to bring change to the European mental health care system, and to remedy the ‘professional intolerance’ of psychosocial disabilities in the community across Europe, by guaranteeing the availability of support for inclusion in its full diversity, and by aborting the doctrine of ‘normalcy’.
Burning issue: COVID 19 and the right to life
The number of preventable deaths of persons with psychosocial disabilities in hospitals, prisons and institutions due to coercion, violence and neglect, has always been strikingly high even before the recent Covid-19 pandemic. Currently, this emergency crisis situation clearly shows that institutions are not safe places. On the contrary, they are places of isolation, loneliness, risk and death. The Covid-19 pandemic sharpens the need for deinstitutionalization and true protection of the human rights of persons with psychosocial and other disabilities, as opposed to the widespread deprivation of rights and liberties through institutionalization and forced treatments under the pretext of health care.
Discriminatory sequence under Article 5.1.e of the European Convention on Human Rights
There is clearly a clash between the human rights enshrined in CRPD article 14 on Liberty and security of the person, and the provisions of Article 5.1.e of the European Convention on Human Rights. The impact of the COVID-19 pandemic on people in institutions proves that the first part of ECHR article 5.1.e regarding the “lawful detention of persons for the prevention of the spreading of infectious diseases” cannot be maintained since it does not protect the human rights of those concerned. The second part of ECHR 5.1.e concerning detention “of persons of unsound mind” is countered and superseded by the CRPD. The third part of ECHR 5.1.e on detention of “drug addicts, alcoholics and vagrants” should be dealt with under regular civil and criminal law, and the provision of shelter and support should be provided in line with the CRPD. Therefore, article 5.1.e is outdated and obsolete, and must be repealed and amended by the provisions of Article 14 of the UN Convention on the Rights of Persons with Disabilities, and in adherence to article 53 of the Vienna Convention on the Law of Treaties of 1980.
The provisions under the Council of Europe’s Oviedo Convention on Human Rights and Biomedicine, dating from 1997, article 6 and 7 are similarly based on the deprivation of rights, and not on the provision of support. These two European Conventions have set the tone of the European interpretation of human rights and mental health for too many years, by legitimizing widespread detention and coercion and presenting these harmful methods as supposed solutions under the “right to health”.
The Draft Additional Protocol to the Oviedo Convention now presents another framework of the same kind in more detail, with a similar repressive approach to mental health crisis situations, which is in violation of CRPD article 14. As history with the ECHR 5.1.e. has already shown us, the provisions entailed by the Draft Additional Protocol to the Oviedo Convention would only be leading to forced hospitalization and treatment, community treatment orders, guardianship and institutionalization in Europe.
Opposing the Council of Europe’s Draft Additional Protocol to the Oviedo Convention
Unfortunately, at present the Council of Europe has still been working on their Draft Additional Protocol to the Oviedo Convention, which is still based on the old notion of repressive psychiatry and is focusing on “involuntary treatment and placement of persons unable to consent”. This development runs counter to the UN CRPD and the ignorant position of the Council of Europe’s Bioethics Committee is absolutely shocking considering the course of history. The ongoing neglect of the European mental health sector is unacceptable.
Over the past decade, a growing number of international organizations and human rights experts have expressed their deep concerns over the development of the Draft Additional Protocol to the Oviedo Convention, and have pushed for its withdrawal. In 2018, the UN CRPD Committee has issued a public statement calling on the state parties of the Council of Europe to vote against the Draft Additional Protocol to the Oviedo Convention.
Yet the Council of Europe’s Bioethics Committee has still not changed their approach.
In June 2021 the Draft Additional Protocol to the Oviedo Convention will be put to a vote at the Bioethics Committee of the Council of Europe, for final adoption at the end of 2021 or early 2022 by the Council of Europe’s Committee of Ministers which has the final decision making power.
Join the campaign!
It is very important to raise awareness on the human rights concerns in regards to European mental health care. Please help us to convince European leaders to vote against the Draft Additional Protocol to the Oviedo Convention.
To join the campaign against the Council of Europe’s Draft Additional Protocol to the Oviedo Convention, please visit the campaign website https://www.withdrawoviedo.info/join or find out more at http://enusp.org
Conclusion
Even while the exact scope of MK Ultra may not be clarified yet, history up to today contains enough lessons to be learned. Efforts must be made to end institutionalization and forced treatments, and European governments must take action, now.
What is needed in Europe:
- Immediate abolition of torture and ill-treatment
It must be recalled that the abolition of torture is not subject to progressive realization, but requires immediate realization. The abolition of coercion in mental health care must be prioritized, and a transformation must be made urgently to scale up supportive systems which ensure all fundamental human rights and freedoms on an equal basis with others. Only good, non-coercive practices should be legal in Europe.
- Moratorium on forced treatments, institutionalization and guardianship
In light of the Council of Europe Member States’ human rights obligations under the UN CRPD, Council of Europe instruments should no longer be used as grounds for detention of persons with disabilities. Instead, a moratorium on forced admissions, on the use of seclusion and restraint, the administration of forced medication, forced interventions of all types and substitute decision-making must be instituted with due urgency.
- Replace discriminatory laws, including ECHR 5.1.e, by UN CRPD-based legislation
The Council of Europe’s Draft Additional Protocol to the Oviedo Convention must be stopped. The sequence of harmful legislation allowing for coercion and institutionalization must be repealed. The UN Convention on the Rights of Persons with Disabilities should guide Europe to respect the human rights of persons with disabilities.
Coercion is not care.
Visit https://www.withdrawoviedo.info/join for campaign materials against the Council of Europe’s Draft Additional Protocol to the Oviedo Convention.
Attachment: Scope of MK Ultra
One 1955 MKUltra document, attached to the US Senate MKUltra Hearing in 1977, gives an indication of the size and range of the effort. It refers to the study of an assortment of mind-altering substances described as follows:
- Substances which will promote illogical thinking and impulsiveness to the point where the recipient would be discredited in public.
- Substances which increase the efficiency of mentation and perception.
- Materials which will prevent or counteract the intoxicating effect of alcohol.
- Materials which will promote the intoxicating effect of alcohol.
- Materials which will produce the signs and symptoms of recognized diseases in a reversible way so they may be used for malingering, etc.
- Materials which will render the induction of hypnosis easier or otherwise enhance its usefulness.
- Substances which will enhance the ability of individuals to withstand privation, torture, and coercion during interrogation and so-called “brain-washing”.
- Materials and physical methods which will produce amnesia for events preceding and during their use.
- Physical methods of producing shock and confusion over extended periods of time and capable of surreptitious use.
- Substances which produce physical disablement such as paralysis of the legs, acute anemia, etc.
- Substances which will produce “pure” euphoria with no subsequent let-down.
- Substances which alter personality structure in such a way the tendency of the recipient to become dependent upon another person is enhanced.
- A material which will cause mental confusion of such a type the individual under its influence will find it difficult to maintain a fabrication under questioning.
- Substances which will lower the ambition and general working efficiency of men when administered in undetectable amounts.
- Substances which promote weakness or distortion of the eyesight or hearing faculties, preferably without permanent effects.
- A knockout pill which can be surreptitiously administered in drinks, food, cigarettes, as an aerosol, etc., which will be safe to use, provide a maximum of amnesia, and be suitable for use by agent types on an ad hoc basis.
- A material which can be surreptitiously administered by the above routes and which in very small amounts will make it impossible for a person to perform physical activity.



{kind=link}